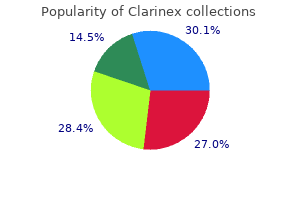
Clarinex
"5 mg clarinex for sale, allergy link".
By: C. Leon, M.B. B.A.O., M.B.B.Ch., Ph.D.
Clinical Director, College of Osteopathic Medicine of the Pacific, Northwest
T4 can be thought of as the precursor to T3; deiodonases (enzymes that remove iodine from a molecule) are located in target tissues and convert T4 to T3 allergy testing buffalo ny purchase clarinex 5 mg online. They accelerate cholesterol clearance from the plasma and increase the rate of glucose absorption from the small intestine allergy testing york region buy discount clarinex 5 mg on line. Excessive thyroid hormone levels (hyperthyroidism) can cause rapid weight loss, anxiety, jitteriness, and fever. Describe the primary metabolic function of each of the following hormones: Insulin: Glucagon: Cortisol: Catecholamines: Thyroid hormones (T3/T4): 2. Thyroid storm is a potentially lethal state of extreme hyperthyroidism in which T3 and T4 levels are significantly above normal limits. The major sites of metabolic activity in the body are the liver, skeletal and cardiac muscles, brain, and adipocytes. Connective tissue and epithelial cells do not make major contributions to the consumption of energy. Remember though, that epithelial cells are the primary secretory cells, so they are involved in the regulation of metabolism. The organ-specific patterns of fuel utilization in the well-fed and fasting states are summarized in Table 12. Organ Liver Resting skeletal muscle Cardiac muscle Adipose tissue Brain Red blood cells Well-Fed Glucose and amino acids Glucose Fatty acids Glucose Glucose Glucose Fasting Fatty acids Fatty acids, ketones Fatty acids, ketones Fatty acids Glucose (ketones in prolonged fast) Glucose Table 12. Any glucose remaining in the liver is then converted to acetyl-CoA and used for fatty acid synthesis. The increase in insulin after a meal stimulates both glycogen synthesis and fatty acid synthesis in the liver. In the well-fed state, the liver derives most of its energy from the oxidation of excess amino acids. Lactate from anaerobic metabolism, glycerol from triacylglycerols, and amino acids provide carbon skeletons for glucose synthesis. Lipoprotein lipase, an enzyme found in the capillary bed of adipose tissue, is also induced by insulin. The fatty acids that are released from lipoproteins are taken up by adipose tissue and re-esterified to triacylglycerols for storage. The glycerol phosphate required for triacylglycerol synthesis comes from glucose that is metabolized in adipocytes as an alternative product of glycolysis. During the fasting state, decreased levels of insulin and increased epinephrine activate hormone-sensitive lipase in fat cells, allowing fatty acids to be released into the circulation. After a meal, insulin promotes glucose uptake in skeletal muscle, which replenishes glycogen stores and amino acids used for protein synthesis. In the fasting state, resting muscle uses fatty acids derived from free fatty acids circulating in the bloodstream. Active Muscle the primary fuel used to support muscle contraction depends on the magnitude and duration of exercise as well as the major fibers involved. Short bursts of high-intensity exercise are also supported by anaerobic glycolysis drawing on stored muscle glycogen. During moderately high-intensity, continuous exercise, oxidation of glucose and fatty acids are both important, but after 1 to 3 hours of continuous exercise at this level, muscle glycogen stores become depleted, and the intensity of exercise declines to a rate that can be supported by oxidation of fatty acids. Slow-twitch muscle fibers in arm and leg muscles are well vascularized and primarily oxidative. Slow-twitch fibers and the number of their mitochondria increase dramatically in trained endurance athletes. Thus, not surprisingly, cardiac myocytes most closely parallel skeletal muscle during extended periods of exercise. In patients with cardiac hypertrophy (thickening of the heart muscle), this situation reverses to some extent. Blood glucose levels are tightly regulated to maintain a sufficient glucose supply for the brain (and sufficient concentration while studying). In hypoglycemic conditions hypothalamic centers in the brain sense a fall in blood glucose level, and the release of glucagon and epinephrine is triggered. Fatty acids cannot cross the bloodbrain barrier and are therefore not used at all as an energy source. Between meals, the brain relies on blood glucose supplied by either hepatic glycogenolysis or gluconeogenesis.
The single needle electrode food allergy treatment guidelines order clarinex without prescription, cluster electrode allergy medicine 9\/3 order 5 mg clarinex with mastercard, single microwave antennae, and single cryoprobe produce a coagulation zone that is nearly circular in cross-section and ellipsoid in the coronal plane. The Starburst multitined expandable electrode generates a teardrop shape ablation with deformations that correspond to the expandable tines. Chemical ablation produces an unpredictable ablation because it is dependent on diffusion at injection and the degree of tumor encapsulation. Patients can be discharged home if they are hemodynamically stable and have recovered from sedation to the point of tolerating oral intake and passing urine 2-4 hours after ablation. Some patients are admitted for observation to manage coexisting morbidity, the effects of anesthesia, or for continued analgesia management. It appears that the number of ablations correlates better with the postablation symptoms than with the maximal diameter of the Adjunctive Techniques to Protect Organs A number of techniques have been developed to protect adjacent organs or structures from the zone of ablation. Perfusion of the biliary tree has been described to protect the central bile ducts when they are within 6 mm of the ablation zone, but this has not been extensively evaluated. Adjuvant Therapies Local therapy combined with transarterial chemoembolization or systemic drug therapy can have additive effects on local tumor control and survival (Box 28-2). Thermal ablation using heat leads to sensitization of the cells to chemotherapeutic agents at the periphery of the tumor which have not undergone coagulative necrosis. D, Noncontrast computed tomography scan after alcohol ablation demonstrates a low-density zone (arrow) adjacent to the tip of a radiofrequency electrode that was used to complete the ablation of the inferior margin. The risk of abscess formation is increased if the patient had recent biliary instrumentation, biliary bypass surgery, bilioenteric fistula, biliary external drainage, or obstruction of the biliary tree. Open cryoablation has been associated with liver fracture, intraperitoneal hemorrhage, and disseminated intravascular coagulation and multiorgan failure (1%). It has been associated with development of arrhythmias and must be performed with general anesthesia and muscle relaxation due Flulike symptoms and fever Low-grade fever that ranged from 99° to 102°F (37°C-39°C) Flulike symptoms: Nausea Vomiting Malaise Myalgia to muscle stimulation and pain secondary to the high-voltage application. The liver is assessed for residual enhancement in the treated tumor, size of the zone of ablation, and development of new metastatic disease. Image-guIded ablatIon of lIver tumors 579 Residual disease is defined as persistent enhancement in an area or areas of tumor after ablation, as determined on the 1- or 3-month follow-up study. A thin homogenous rim of peripheral enhancement has been shown to represent evolving granulation tissue and should not be mistaken for residual tumor. A common interpretive pitfall by those unfamiliar with postablation imaging is to report tumor enlargement on the first postablation scan when in fact what has occurred is development of a zone of ablation larger than the original tumor, a desirable result. On subsequent follow-up scans, after absence of viable tumor at imaging has been confirmed once, the zone of ablation may stay the same size or slowly decrease in size. Local progression of disease or recurrence is defined as new tumor enhancement after at least one imaging study has demonstrated complete elimination of enhancement. If new tumors develop, then reevaluation can be performed as to whether percutaneous ablation and/or other locoregional or systemic therapies are warranted. Large-volume tissue ablation with radio frequency by using a clustered, internally cooled electrode technique: laboratory and clinical experience in liver metastases. Risk factors for distant recurrence of hepatocellular carcinoma in the liver after complete coagulation by microwave or radiofrequency ablation. Small hepatocellular carcinoma in cirrhosis: randomized comparison of radio-frequency thermal ablation versus percutaneous ethanol injection. Large liver tumors: protocol for radiofrequency ablation and its clinical application in 110 patients - mathematic model, overlapping mode, and electrode placement process. Randomized clinical trial of percutaneous radiofrequency ablation plus absolute ethanol injection compared with radiofrequency ablation alone for small hepatocellular carcinoma. Percutaneous radiofrequency ablation of ovarian cancer metastasis to the liver: indications, outcomes, and role in patient management. Ultrasound-guided percutaneous ethanol injection under general anesthesia for the treatment of hepatocellular carcinoma on cirrhosis: long-term results in 268 patients. Thoracic and neck the aorta emerges from the left ventricle at the lower border of the third costal cartilage behind the sternum (slightly to the left). In the superior mediastinum it curves upwards, backwards and to the left, forming in turn the ascending aorta, aortic arch and then the descending thoracic aorta. The outer convexity of the aortic arch gives three branches: 1 Brachiocephalic (which is short and quickly divides into the right common carotid and right subclavian). On each side then, the common carotid artery ascends in the neck almost and identically passing behind (although very deeply) the sternoclavicular joint to the upper border of the thyroid where it divides into the external carotid and internal carotid. Meanwhile, the descending thoracic aorta passes through the thorax on the vertebral column, giving various branches in the mediastinum.
Another variant displays focal to extensive areas resembling Sertoli and Sertoli-Leydig cell tumours 1431 allergy asthma and immunology generic clarinex 5mg without prescription,1638 allergy symptoms wheat intolerance generic 5mg clarinex otc,2117. Furthermore, the stroma may appear cellular and fibrous, resembling the spindle cell component of stromal tumours. These tumours are designated as "sertoliform Endometrioid tumours 31 endometrioid carcinoma" or "endometrioid carcinoma resembling sex cord-stromal tumour". On occasion, foci indistinguishable from moderate to poorly differentiated squamous carcinoma can be seen. Grading the grading of endometrioid carcinoma of the ovary is the same as for endometrial adenocarcinoma of the uterus. Poorly differentiated endometrioid carcinomas are predominantly solid with focal microglandular areas. Distinguishing high-grade endometrioid carcinoma from high-grade serous carcinoma may be difficult and immunohistochemical staining more characteristic of serous carcinoma may aid in this distinction. The histogenesis of high-grade endometrioid carcinoma is not as clear, since many tumours that have been classified as such in the past, probably are high-grade serous carcinomas showing glandular differentiation. Genetic profile -catenin-mediated canonical Wnt pathway signalling is dysregulated in 1638% of endometrioid carcinomas 1300,1665, 2050,2054,2055. The mutations are typically frameshift or nonsense mutations that result in loss of protein expression. However, more recent studies indicate that many ovarian tumours previously diagnosed as high-grade endometrioid carcinomas lack mutations characteristic of lowgrade endometrioid carcinoma and have gene expression profiles indistinguishable from high-grade serous carcinomas 1704,2054. Peritoneal foreign body granulomas containing keratin have been found in cases of endometrioid carcinomas with squamous differentiation do not affect the prognosis adversely in the absence of viable-appearing tumour cells and do not warrant upstaging 925. Endometrioid carcinoma of the ovary associated with carcinoma of the endometrium occurs in 1520% of cases 523,946,1755,2142. The criteria for distinguishing metastatic from independent primary carcinomas rely mainly on the clinicopathological findings. In these patients, however, the 5-year survival is 7092%, and the median survival is 10 years or longer 1807,1849; thus, follow-up favours two independent adenocarcinomas since most patients survive without recurrence 523,1481,1522. In contrast, bilaterality and multinodular growth, as well as vascular space and tubal invasion, are characteristic of ovarian metastases. Zhou Clear cell cystadenoma / adenofibroma Definition A tumour composed of glands or cysts lined by bland cuboidal to flattened cells with clear or eosinophilic cytoplasm embedded in a fibromatous stroma. Macroscopy Adenofibromas form a solid mass ranging from 316 cm, with a smooth, lobulated external surface and on sectioning, small cysts can be seen within a solid background. Histopathology In adenofibromas, widely spaced simple glands, often cystically dilated, are embedded in a fibromatous stroma. The glands are lined by cells that can be cuboidal to flattened, with clear or eosinophilic cytoplasm. The rare cystadenomas have bland lining cells that at least focally have clear cytoplasm but are often compressed with scant cytoplasm. All tumours have been confined to the ovaries and almost all are unilateral 122,874,1952,2164. On sectioning, they are solid but may contain tiny cysts; rarely, large cysts are seen 122,1636,1867,2164. Histopathology the glands are typically round to oval and relatively evenly spaced in a fibromatous stroma. Some degree of compaction of glands may be evident but stromal invasion, and hence small foci of invasive clear cell carcinoma, should only be diagnosed when a clearly abnormal architecture indicative of invasion, sometimes associated with a stromal reaction, is present. The cysts and glands are lined by cuboidal, hobnail, or flattened cells with clear or eosinophilic cytoplasm. Clear cell borderline tumour / Atypical proliferative clear cell tumour Definition these are clear cell adenofibromatous tumours with atypia of the glandular epithelium but without stromal invasion. Clear cell tumours 33 Prognosis and predictive factors All well documented cases have been benign 122,1867,1952. Clear cell carcinoma Definition A malignant tumour composed of clear, eosinophilic and hobnail cells, displaying a combination of tubulocystic, papillary and solid patterns. Clear cell carcinoma accounts for a higher percentage of ovarian carcinomas in Japan relative to western countries 264,821,1856. Clinical features Clear cell carcinoma is the ovarian tumour most frequently associated with ovarian or pelvic endometriosis 393,584, 1316,1408.
Syndromes
- Pregnant teens and women: 15 mg/day
- Urine tests to see what may be causing dehydration
- Severe change in blood acid levels -- leads to organ damage
- Serum prolactin levels
- Bladder cancer
- Intimacy and sexuality
The most important factor predicting lymph node metastases is tumour depth and the strongest correlate of outcome is lymph node status 2040 allergy forecast in san antonio buy genuine clarinex line,2090 allergy forecast in nyc purchase clarinex 5mg line. This tumour contains demarcated nests of palisaded basal cells originating at the epidermaldermal junction. Benign squamous lesions Basal cell carcinoma Definition An infiltrating tumour composed predominantly of cells resembling the basal cells of the epidermis. Macroscopy Papular or warty lesion may be seen on the introital, labial, perineal, and perianal mucosa. Histopathology Acanthosis, papillomatosis, hyperkeratosis, parakeratosis, parabasal hyperplasia, delayed maturation and variable superficial (koilocytotic) atypia may be seen. In keratinized epithelium, koilocytotic atypia is not required for this diagnosis if the other criteria are present. Prognosis and predictive factors the disease is managed by observation, local excision, topical imiquimod or trichloroacetic acid, and electro-cautery or superficial cryotherapy when larger. Histopathology this tumour is composed of aggregates of uniform basal cells with peripheral palisading. Half are infiltrative and a minority contains gland-like structures (adenoid basal cell carcinoma). Those containing infiltrating malignant-appearing squamous cells may be diagnosed as metatypical basal cell carcinoma or basosquamous carcinoma and should be managed similarly to squamous cell carcinoma 930. The differential diagnosis of basal cell carcinoma also includes benign trichogenic tumours (trichoepithelioma). Histogenesis this tumour is derived from the basal cells of the epidermis or hair follicles. Acanthosis and papillomatosis with only focal viral cytopathic effect (centre right near the surface). Definition A benign epithelial excrescence with a squamous epithelial mucosal surface that overlies a delicate fibrovascular stalk. Clinical features Keratoacanthomas have been reported to arise rapidly, in some instances associated with prior trauma 1473. Macroscopy Keratoacanthomas present as non-ulcerated lumps or nodules, typically 12 cm in diameter. Histopathology Keratoacanthomas are discrete, inverted, and form a crater of well differentiated keratinocytes with a resemblance to pseudoepitheliomatous hyperplasia. Prognosis and predictive factors Some regress spontaneously and most vulvar lesions have an uneventful outcome. However, many lesions classified as keratoacanthomas demonstrate some atypia and metastases have been reported. In this situation, the tumour is referred to as squamous cell carcinoma, keratoacanthoma type 765. Synonyms Micropapillomatosis labialis; vestibular micropapillomatosis; hirsuties papillaris genitalis (these terms are applicable when numerous frond-like excrescences are present) Clinical features the lesions may be solitary but frequently are multiple, often occurring in clusters near the hymenal ring and within the vulvar vestibule: this is termed vestibular papillomatosis or micropapillomatosis labialis. They do not display acanthosis or atypia and should not be treated as or mistaken for condyloma 137. Histopathology these lesions have a papillary architecture and a smooth surface without acanthosis or koilocytotic atypia. The most plausible explanation is a simple variant of mucosal anatomy in the vulvar vestibule 1262. Clinical features the lesion is usually red, eczematoid, pruritic and may clinically resemble a dermatosis 529. Paget disease of anorectal origin involves the perianal mucosa and skin as well as the adjacent vulva. Histopathology Large round "Paget cells" with prominent pale cytoplasm and a prominent central nucleolus are distributed throughout the epithelium, either as single cells or clusters with variable extent. Histogenesis Paget disease is an epithelial neoplasm arising from pluripotent epidermal stem cells, residing in interfollicular epidermis and in the folliculo-apocrine-sebaceous units. It may also be derived from an underlying skin appendage adenocarcinoma or anorectal or urothelial carcinoma 2030. Seborrheic keratosis Definition A benign tumour characterized by proliferation of the parabasal cells of the squamous epithelium. Histopathology Acanthosis, hyperkeratosis and the formation of keratin-filled pseudohorn cysts may be seen.